Fechtner syndrome is a rare inherited condition caused by a change in a single gene called MYH9. It is passed down through families in what doctors call an “autosomal dominant” pattern — meaning you only need to inherit the changed gene from one parent to be affected.
But there is something critical to know: approximately 30–35% of people with this condition are the first in their family to have it. The change happened new, just in them. So not having a family history does not rule this out.
Today, Fechtner syndrome is understood to be one presentation of a broader condition called MYH9-Related Disease (MYH9-RD). Think of it as a spectrum — like different shades of the same color — ranging from mild to more serious. Fechtner syndrome represents the end of the spectrum where more organ systems are involved: blood, kidneys, hearing, eyes, and sometimes liver.
The estimated prevalence is approximately 1 in every 20,000–25,000 people worldwide. Because it is so often mistaken for other conditions, the true number of people living with it is almost certainly higher than the records show.
TC
Thomas CheesmanFounder, Bare Your Rare · Rare disease patient
Symptoms — What to Watch For
Not every person gets every symptom. Some people live their whole lives with only the blood abnormality. Others develop kidney, hearing, or eye problems over time. The same gene change can affect people very differently, even within the same family.
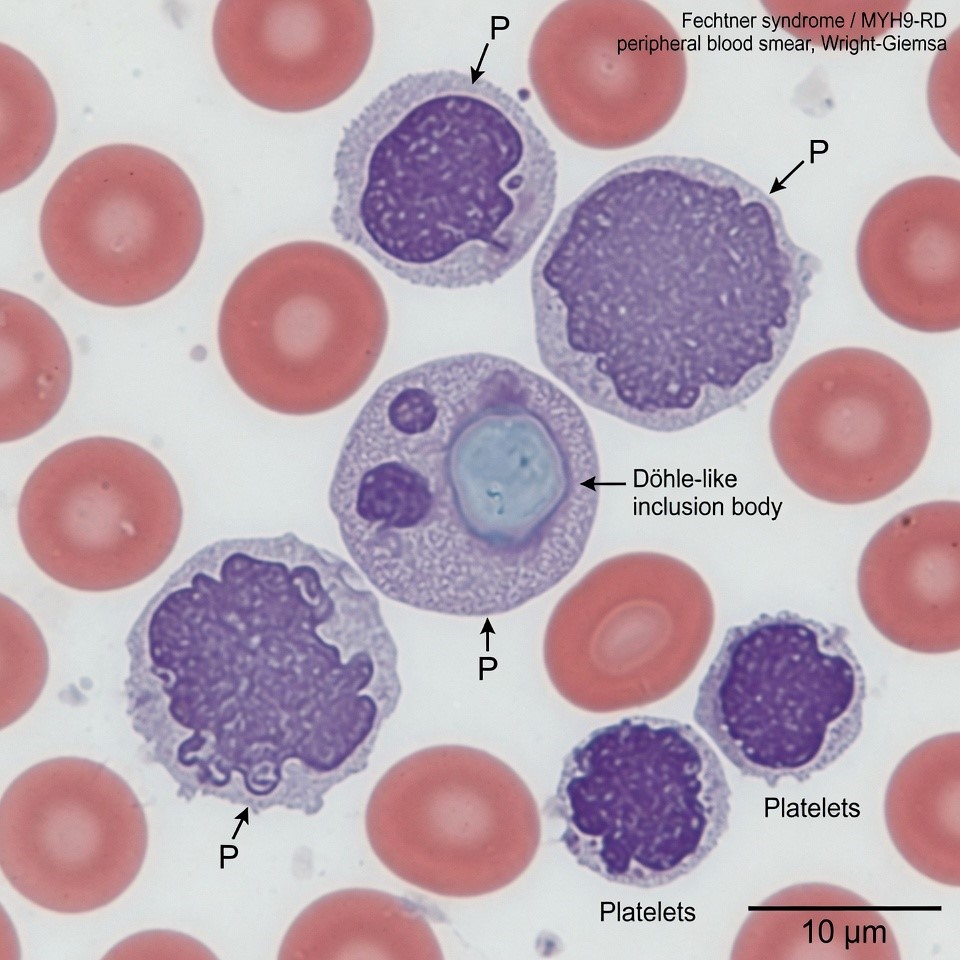
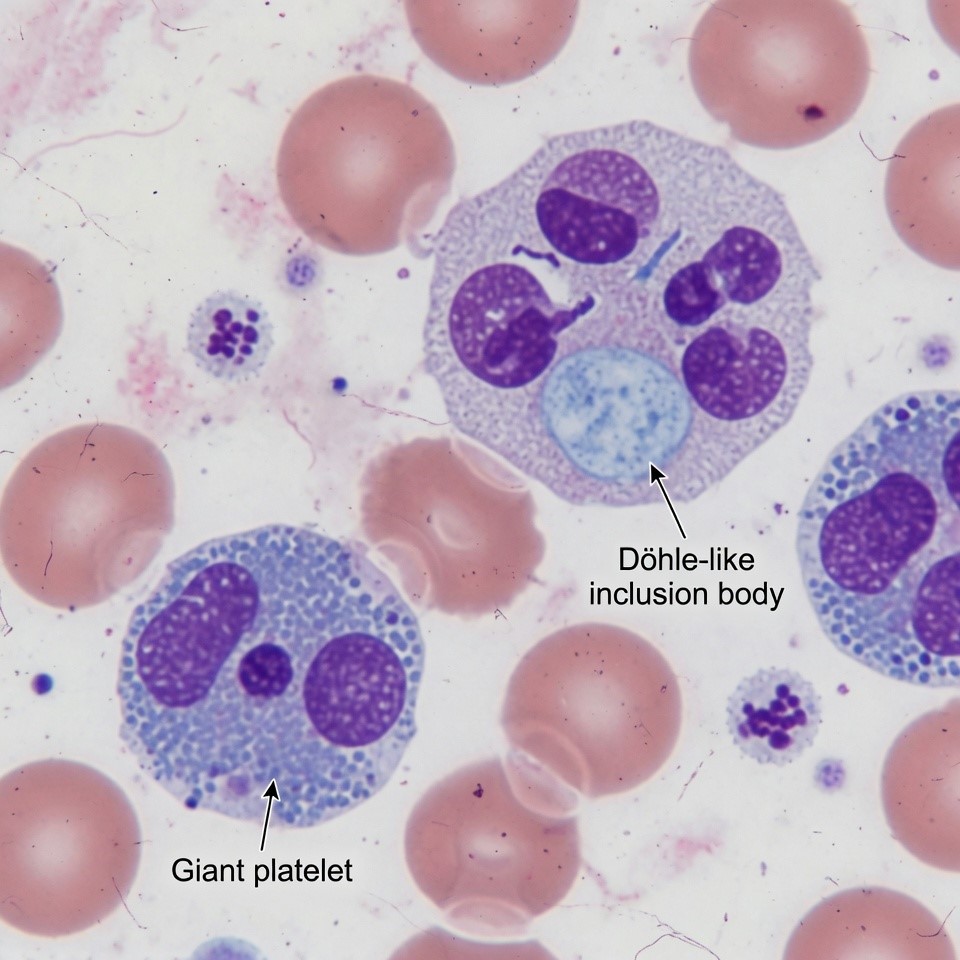
The body produces too few platelets, and the ones it makes are abnormally large — sometimes as big as a red blood cell. White blood cells also carry tiny spots inside them called Döhle-like inclusion bodies. This is actually a valuable clue for diagnosis.
Döhle-like inclusion bodies in neutrophils — a key diagnostic clue
What you might notice
Easy bruising, nosebleeds that take longer to stop than they should, heavier-than-usual periods in women, or longer bleeding after cuts or dental work. Life-threatening bleeding is rare in everyday life, but surgical procedures and deliveries require careful advance planning.
The kidney’s filtering system is gradually damaged. About 75% of patients who develop kidney involvement show signs before age 35, though it can appear at any point in life. Without treatment, progression to kidney failure is common.
What you might notice
Protein or blood in the urine (often found on a routine urine test before you feel any symptoms), rising blood pressure, or increasing tiredness over time. Early detection and treatment can significantly slow this down.
Gradual high-frequency hearing loss is one of the most common features. Onset can happen anywhere from childhood to the sixth decade of life, and severity ranges from very mild to profound deafness.
What you might notice
Difficulty hearing high-pitched sounds, asking people to repeat themselves, or needing the TV louder than others prefer. This typically gets worse slowly over time.
Cataracts — clouding of the lens — usually appear in early adulthood, though they have been reported in children. They are often present in both eyes.
What you might notice
Blurry or foggy vision, increased glare sensitivity, or difficulty seeing at night. Standard cataract surgery is effective.
Elevated liver enzymes are now a recognized feature of MYH9-RD. Most patients do not feel any symptoms from this, and it is typically found on a routine blood panel. Serious liver disease is not a common outcome, but it is something your doctors should monitor.
What you might notice
Usually nothing — this is discovered on lab work.
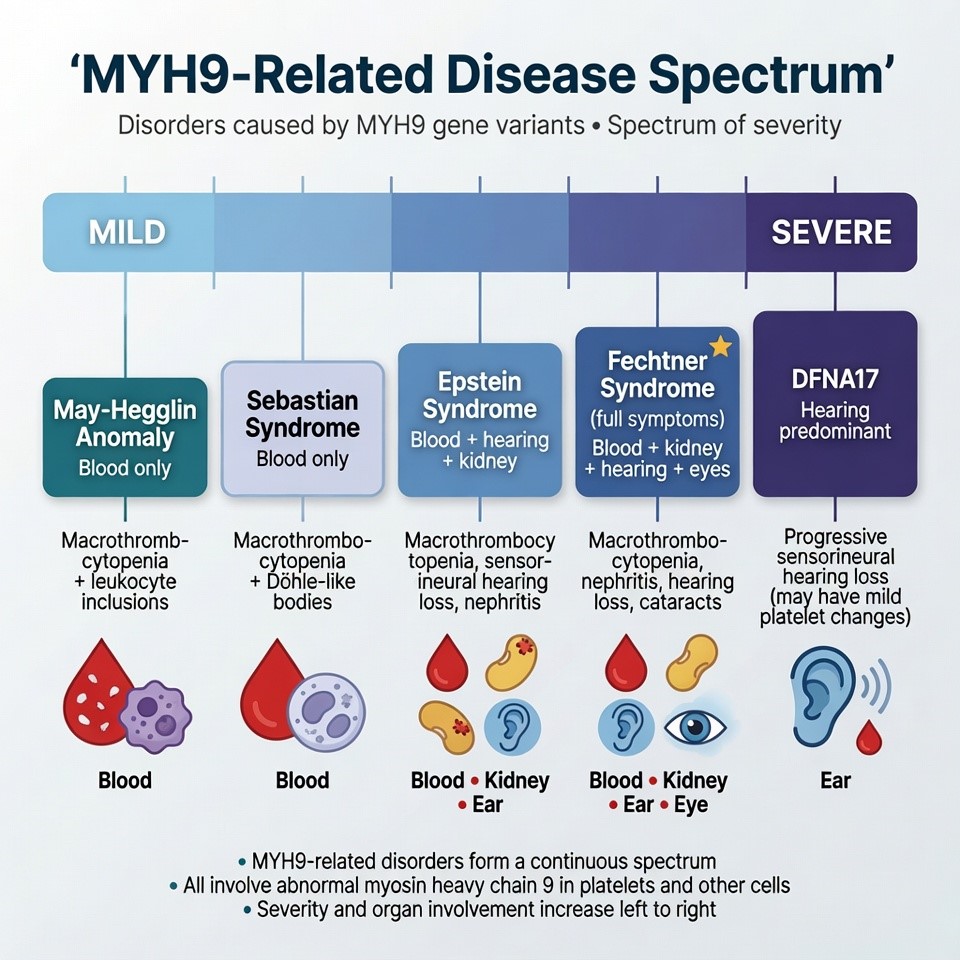
The Full Spectrum — Five Conditions, One Disease
What used to be called five separate conditions are now understood to be different expressions of the same underlying MYH9 gene change:
The MYH9-Related Disease spectrum — one gene, five historical names
Mildest
May-Hegglin Anomaly
Blood changes only (giant platelets, inclusions). The mildest presentation.
Sebastian Syndrome
Same blood changes; inclusions have a slightly different appearance under electron microscopy.
Epstein Syndrome
Blood changes plus kidney disease and hearing loss, but no leukocyte inclusions on standard staining.
You Are Here
Fechtner Syndrome
Blood changes, inclusions, kidney disease, hearing loss, and cataracts. The most complete presentation.
Recently added
DFNA17
Initially classified as hearing loss alone, now confirmed to be part of the MYH9-RD family.
Why the Label Matters Less Than You Think
The label a doctor uses often depended on which symptoms appeared first and how the patient was examined. Because the condition evolves over time, someone may start with what looks like May-Hegglin and later develop features of Fechtner syndrome.
A Brief History of How We Got Here
1985
First Description
Dr. L.C. Peterson and colleagues publish the first description of the Fechtner family in Blood. Eight members across four generations are affected.
1988
Second Family Documented
A second family is confirmed, establishing the syndrome as real and recurring.
2000
MYH9 Gene Identified
The May-Hegglin/Fechtner Syndrome Consortium identifies MYH9 mutations as the shared cause, linking multiple syndromes as one disease.
2001–03
Spectrum Unified
Epstein syndrome confirmed to share the same genetic cause. The term MYH9-Related Disease (MYH9-RD) is proposed.
2008
Kidney Protection Confirmed
First study confirms that ACE inhibitors and ARBs reduce kidney damage in MYH9-RD patients (Pecci et al.).
2010
Eltrombopag Breakthrough
Eltrombopag shown to effectively raise platelet counts. Cochlear implants confirmed safe and effective for hearing loss.
2014
Prognostic Model Published
Landmark study shows where in the MYH9 gene the mutation sits predicts the likely course of the disease.
2020
Mechanism Deepened
Research confirms that megakaryocyte migration defects underlie the thrombocytopenia.
2024–25
Misdiagnosis Crisis Exposed
Multiple studies confirm widespread misdiagnosis. Avatrombopag emerges as an alternative. A 2025 case report confirms MYH9-RD can present with normal platelet counts.
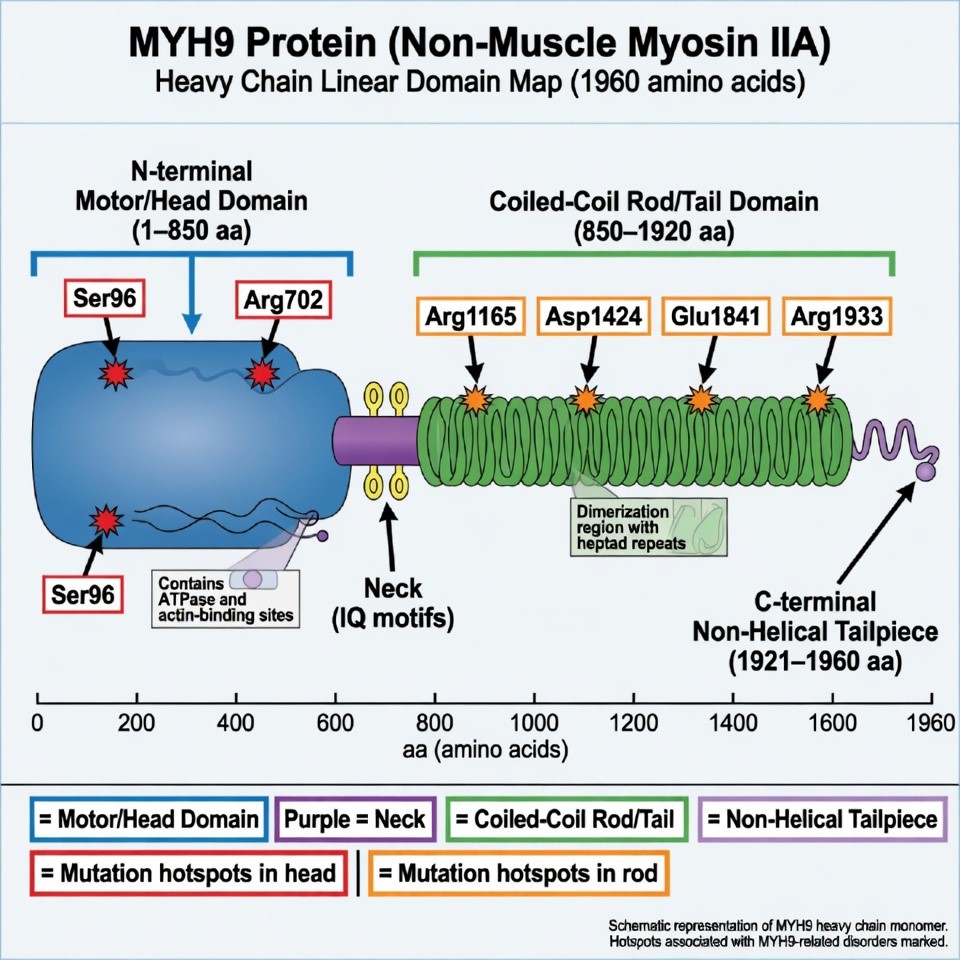
The MYH9 gene sits on chromosome 22 and provides the instructions for making a protein called non-muscle myosin IIA (also called myosin-9). Think of this protein as a tiny molecular motor inside your cells — it helps cells hold their shape, divide properly, and move internal materials around.
This motor is especially important in three places:
The MYH9 protein — head domain vs. tail domain, with key mutation sites
🩸
Bone marrow cells (megakaryocytes)
That make platelets
🫀
Kidney filter cells (podocytes)
Essential for proper filtration
👂
Inner ear & eye lens cells
Sensory cell maintenance
When the MYH9 gene has a mutation, the motor doesn’t work right. In blood cells, it causes platelets to be released too early, too large, and too few of them. In kidney cells, it weakens the filter. In the inner ear and eyes, it leads to gradual deterioration.
Where the Mutation Sits Matters
The gene has two main regions — a “head” (motor) region and a “tail” region. About 70% of all known mutations affect just six specific amino acid positions.
Head / Motor Domain
Especially positions Ser96 & Arg702
Higher risk of kidney failure and more severe hearing loss. This is classic Fechtner syndrome territory.
Tail / Coiled-Coil Domain
Positions Arg1165, Asp1424, Glu1841, Arg1933
Often milder overall, with the kidney disease developing later or not at all.
Why This Matters for You
This information helps doctors predict what to watch for in each individual patient, and how often to screen for kidney, hearing, and eye changes.
The most important first step is a peripheral blood smear reviewed by an experienced eye. Electronic cell counters often miss or undercount the giant platelets of MYH9-RD because the machine doesn’t recognize them as platelets. A human looking through a microscope is essential.
Döhle-like inclusion bodies under immunofluorescence — the most reliable diagnostic sign
1
Complete Blood Count
Will show low platelet count (though occasionally normal) and may not capture the giant platelet size accurately.
2
Peripheral Blood Smear
A slide of blood viewed under a microscope. The doctor looks for giant platelets and faint pale-blue Döhle-like inclusion bodies in neutrophils.
3
Immunofluorescence Staining
A more sensitive test that stains for the MYH9 protein in neutrophils. This is considered the most reliable diagnostic sign.
4
MYH9 Genetic Testing
Confirms the specific mutation and its location, which helps predict the course of the disease.
⚠ The Misdiagnosis Crisis
The low platelet count looks identical to immune thrombocytopenic purpura (ITP) on a standard blood count. Doctors often start treating for ITP with steroids or immunosuppressants, which do nothing for MYH9-RD. Some patients go years — even 10–17 years — before someone looks at a blood smear and notices the giant platelets and inclusion bodies.
MYH9-RD cases are frequently misdiagnosed, leading to unnecessary treatments such as corticosteroids, immunosuppression, or even splenectomy, thus missing optimal treatment opportunities.
🏥 For Nurses and Emergency Staff
If a patient with known MYH9-RD or Fechtner syndrome comes in for any procedure, bleeding episode, or surgery, the platelet count alone is not a reliable guide to bleeding risk. These patients need individualized assessment. Platelet transfusion can be used for active bleeding that cannot be controlled locally, but is not a routine prophylactic measure.
Once diagnosed, patients need a team of specialists working together. The following monitoring schedule is recommended based on current guidelines:
Annual
Blood count & platelet assessment
Annual
Urine test for protein
Proteinuria screening
Annual / 6 mo
Kidney function
Creatinine, eGFR — every 6 months for high-risk mutations
Every 3 yr
Hearing test
Every 3 yr
Eye exam for cataracts
Every 3 yr
Liver enzyme check
Things to Avoid
NSAIDs (aspirin, ibuprofen) — only after careful risk-benefit conversation with your doctor
Nephrotoxic or ototoxic drugs — always tell every prescribing doctor and dentist about your diagnosis
High-risk activities with significant injury risk
Hazardous noise exposure — use hearing protection
🚨 Before Any Surgery, Dental Procedure, or Delivery
Tell your care team well in advance. Platelet counts may need to be temporarily raised using medications. Never have elective surgery without your hematologist involved in planning.
There is currently no cure for MYH9-RD. Treatment focuses on protecting the organs that are at risk and managing symptoms when they arise.
Critical
Protecting the Kidneys
ACE inhibitors or ARBs (ramipril, lisinopril, losartan) are the most important long-term treatment for anyone showing protein in their urine. They act like a pressure-reducing valve on the kidneys’ filtering system, slowing damage significantly. SGLT2 inhibitors may also be added.
When kidneys fail: dialysis and kidney transplantation both work well in MYH9-RD patients.
Pre-Surgical
Raising Platelet Counts
For most people with MYH9-RD, the low platelet count does not cause serious daily bleeding and does not need treatment. However, before surgery, invasive procedures, or delivery, platelet counts may need to be temporarily raised.
Eltrombopag — oral TPO agonist, start 1–2 weeks before procedures
Avatrombopag — alternative when eltrombopag is insufficient
Romiplostim — injection option
Platelet transfusion — reserved for active uncontrolled bleeding
Desmopressin (DDAVP) — temporary clotting support
Hearing Loss
Hearing aids are effective for mild-to-moderate loss. Cochlear implants are confirmed safe and effective in MYH9-RD patients with good outcomes. Referral to an ENT specialist familiar with rare diseases is worthwhile.
Cataracts
Standard surgical cataract removal works well and is safe with proper platelet management before the procedure.
Liver Enzymes
Currently, monitoring is the main approach. No specific treatment is required unless levels become significantly elevated. Avoid alcohol and other liver-stressing substances.
Important
Pregnancy & Delivery
Pregnancy requires close coordination between hematology and obstetrics. A platelet count of at least 50 × 10⁹/L is generally recommended for delivery. Epidural decisions need case-by-case hematologist involvement. The baby has a 50% chance of inheriting the condition.
Genetic Counseling
Every diagnosed patient and their family members should have access to a genetic counselor. First-degree relatives should be offered testing. Prenatal testing and preimplantation genetic testing are both available once the specific family mutation is identified.
Registries
Genotype-Phenotype Correlation
Large international registries continue to refine which specific mutations lead to which outcomes, making personalized prognosis more accurate. The Italian Registry of MYH9-RD remains one of the most comprehensive datasets in the world.
Drug Research
TPO Receptor Agonist Research
Multiple studies exploring avatrombopag as an alternative and complement to eltrombopag. A 2025 paper documented successful platelet raising after eltrombopag had failed.
Technology
AI-Assisted Diagnosis
A 2024 paper documented the use of advanced slide-reading technology to identify MYH9-RD hallmarks in blood samples that had previously been misread.
Population Studies
Nationwide Registry Research
A 2024 Japanese nationwide survey expanded understanding of the disease’s kidney outcomes and management across diverse populations.
Transplantation
Transplantation Outcomes
A November 2025 case report documented successful kidney transplantation following hemodialysis as a bridge therapy.
Diagnostic
Misdiagnosis Research
A 2025 Chinese retrospective study of 40 patients misdiagnosed as ITP proposed clearer screening algorithms to prevent the problem.
World’s Leading Expert
Dr. Alessandro Pecci, MD, PhD
IRCCS Policlinico San Matteo Foundation & University of Pavia, Italy
Author of the majority of landmark papers on MYH9-RD, including GeneReviews, the 2014 prognostic model, and the eltrombopag clinical trial.
IRCCS Burlo Garofolo & University of Trieste, Italy
Co-author of the GeneReviews MYH9-RD entry. Leading genetics researcher on the molecular basis of the disease.
Dr. Andreas Greinacher, MD
University Medicine Greifswald, Germany
Foundational work on clinical recognition and perioperative management of MYH9-RD.
Shinji Kunishima, MD
Gifu University of Medical Science, Japan
Leading researcher in Asian populations with MYH9-RD and pediatric presentations.
🏥 Primary Research Center
University of Pavia / IRCCS Policlinico San Matteo — Pavia, Italy. The single most productive center globally for MYH9-RD research and home of the Italian Registry. Patients from outside Italy have contacted this center for expert consultation.
Patient Resources & Organizations
📖 GeneReviews — MYH9-RD
The most comprehensive clinical resource, authored by Pecci & Savoia. Free and openly available.
Oral medications that stimulate the bone marrow to produce more platelets. Used before surgeries and procedures.
TPO receptor agonist
The drug class to which eltrombopag, avatrombopag, and romiplostim belong. They mimic thrombopoietin, the hormone that signals the body to make more platelets.
Cochlear implant
A surgically implanted device that can restore functional hearing. Confirmed safe in MYH9-RD patients.
Variable expressivity
The same gene change can cause very different symptoms, even in members of the same family.
Spectrum disorder
A range of presentations of one underlying condition, from mild to severe.
Your Personal Action Checklist
☐ Ask your doctor for a peripheral blood smear — not just a standard blood count
☐ Ask specifically about MYH9 gene testing
☐ Request referrals to a hematologist and nephrologist familiar with rare diseases
☐ Ask whether any family members should also be tested
☐ Make sure every doctor, dentist, and ER knows about your platelet disorder before any procedure
☐ Wear a medical alert bracelet or carry a wallet card
☐ Know your specific mutation — which part of the gene is affected predicts risk
☐ Follow the monitoring schedule (annual kidney tests, hearing and eye exams every 3 years)
☐ Before any surgery or delivery: contact your hematologist at least 2–3 weeks in advance
☐Avoid aspirin and ibuprofen unless your doctor specifically approved them
☐ If planning a pregnancy: speak with both hematologist and OB beforehand
☐ First-degree relatives all have a 50% chance of carrying the gene change
☐ Ask the family member’s specialist about getting tested
☐ A negative family history does not rule out the condition — testing is the only way to know
Sources & Further Reading
This guide draws on peer-reviewed medical literature and trusted rare-disease databases. Because these conditions are rare, much of what is known comes from case reports and small series — the sources below are where to read further and verify with your own clinicians.
Online Mendelian Inheritance in Man (OMIM). MYH9-related macrothrombocytopenia spectrum (#155100).OMIM
Your Story Matters
If you live with Fechtner syndrome or MYH9-Related Disease, your experience can help someone who was just diagnosed last week. Share your journey, your insights, your questions — this page is a living resource, and your voice belongs here.
Your comments, corrections, and stories help keep this resource accurate and useful. All fields except your message are optional.
Community Voices
Stories and insights from the Fechtner / MYH9-RD community will appear here as they are submitted and reviewed. Be the first to share yours.
No stories yet — yours could be the first.
◆ ◆ ◆
You are not alone. You are home.
All content verified against peer-reviewed medical literature including Pecci & Savoia, GeneReviews 2021; Orphanet 2014 (MYH9-RD); Clinical Kidney Journal 2019; PMC 2024 misdiagnosis case series; Springer Renal Replacement Therapy November 2025; Journal of Thrombosis and Haemostasis 2025; Blood (ASH) 2025; Frontiers in Pediatrics 2024; British Journal of Hospital Medicine January 2026.


Community Voices
Stories and insights from the Fechtner / MYH9-RD community will appear here as they are submitted and reviewed. Be the first to share yours.
No stories yet — yours could be the first.