

Building Your Care Team
There are no HCS clinics. There is no published multidisciplinary care guideline. What exists is a pattern from the literature: the patients who do best are the ones who assemble a coordinated team across multiple specialties and make sure those specialists actually talk to each other.
Endocrinologist
Your quarterback for bone health. Manages bisphosphonates, denosumab, or romosozumab. Orders and interprets DEXA scans. Monitors bone turnover markers (CTX, P1NP). In Alberta, for me anyway, I have a Rheumatologist who manages these things for me.
Neurosurgeon / Neurologist
Basilar invagination and Chiari malformation occur in roughly half of HCS patients and can be life-threatening. Needs to be monitoring with periodic imaging even if you're asymptomatic.
Cardiologist
Congenital heart defects and valve disease are documented in HCS. One patient required mitral valve replacement at age 14 and a pacemaker at 18. Echocardiographic monitoring may be essential.
Nephrologist
Polycystic kidney disease appears in an estimated 10% of HCS patients and has progressed to end-stage renal failure in documented cases. Renal ultrasound at diagnosis and periodic monitoring are critical.
Dental Specialist
HCS causes progressive alveolar bone atrophy, severe periodontal disease, and premature tooth loss. Avoid invasive procedures where possible — especially if you're on bisphosphonates.
Audiologist
Hearing loss — both sensorineural and conductive — is a recognized feature of HCS. Annual audiometry catches changes early enough for hearing aid fitting or other intervention.
Respirologist
Thoracic deformities cause restrictive lung disease. Basilar invagination can cause central respiratory arrest. Vocal cord paralysis has also been documented.
Clinical Geneticist
Confirms diagnosis via NOTCH2 exon 34 sequencing. Essential for family planning discussions and coordinating preimplantation genetic testing (PGT-M) if desired.
No single specialist can manage HCS alone. Print your medication list and bring it to every appointment. It sounds basic. It's the most protective thing you can do.
Monitoring Schedule
There is no published surveillance protocol for HCS. The schedule below is derived from the clinical literature and case report recommendations.
DEXA Bone Density Scan
Quantifies osteoporosis severity, tracks treatment response
Bone Turnover Markers (CTX, P1NP)
Tracks osteoclast activity and treatment response
Hand & Foot X-rays
Documents acro-osteolysis progression
Skull Base CT or MRI
Screens for basilar invagination and Chiari malformation
Spine X-ray Series
Compression fractures, kyphosis, scoliosis, cervical instability
Echocardiogram
Valvular disease, congenital defects
Renal Ultrasound + Function Panel
Polycystic kidneys in ~10% of patients
Audiometry
Progressive sensorineural and/or conductive hearing loss
Pulmonary Function Tests
Restrictive lung disease from thoracic deformities
Dental Exam with Panoramic X-ray
Alveolar bone atrophy, periodontal disease, root resorption
Keep a binder. With fewer than 100 known cases, most specialists you see will be encountering HCS for the first time.
Emergency Red Flags
Some HCS complications are slowly progressive. Others aren't. These are the signs that mean you need emergency evaluation.

- Severe sudden headache with neck stiffness, vomiting, or vision changes — may indicate hydrocephalus from basilar invagination
- New weakness, numbness, or coordination loss in arms or legs — spinal cord compression
- Difficulty swallowing or breathing that worsens rapidly — upper airway obstruction or brainstem compression
- Sleep apnea that suddenly worsens — central respiratory arrest from basilar invagination is a documented cause of death
- Chest pain, palpitations, or fainting — cardiac valve disease can worsen unpredictably
- Blood in urine or severe flank pain — may signal renal cyst complication
- New seizures — documented in HCS patients with neurological involvement
- Sudden severe back pain with height loss — vertebral compression fracture
Carry a medical ID or emergency summary card. In an emergency room, the team treating you will almost certainly not know what HCS is.
Surgical & Anesthesia Safety
HCS is classified in anesthesia literature as one of the most difficult airway-related syndromes. Print this section. Bring it.
Airway Challenges — Why Intubation Is Dangerous
Micrognathia, abnormal dentition, short neck, and cervical spine deformities combine to create a textbook difficult airway. Published case reports recommend video laryngoscopy or fibreoptic intubation. Cervical spine instability means neck extension during intubation is dangerous.
Bleeding Risk & Coagulation
NOTCH2 mutations are associated with bleeding risks. The anesthesia literature recommends preoperative coagulation profile assessment and ensuring adequate blood products are available.
Positioning & Fracture Prevention
Severe osteoporosis and joint laxity mean that positioning during surgery can itself cause fractures. Pressure points need extra padding. The surgical team needs to handle positioning gently.
Spinal Surgery — Why HCS Makes It Harder
Spinal surgery in HCS is documented as exceptionally challenging. Distorted anatomy, reduced bone strength making screw fixation unreliable, and osteolysis causing fusion failure are all documented complications.
Respiratory Considerations During Surgery
HCS patients may have severe restrictive lung disease from thoracic deformities. Pulmonary function testing before any planned surgery gives the anesthesia team the data they need.
Share these recommendations with your surgical team before the procedure, not the morning of.
Dental Management — The Bisphosphonate Paradox
HCS attacks your teeth from below. The alveolar bone progressively atrophies, causing severe periodontal disease and premature tooth loss.

Here's the paradox: bisphosphonates — the most commonly prescribed medications for HCS osteoporosis — carry a known risk of osteonecrosis of the jaw (ONJ).
What the Literature Recommends
Preserve — Don't Extract
The literature explicitly recommends avoiding invasive dental procedures where possible. Conservative restorations are preferred over extractions.
Bisphosphonate-Jaw Risk Coordination
If you're on bisphosphonates, your dentist must know before any invasive procedure. Timing relative to bisphosphonate dosing matters.
Frequent Monitoring Protocol
Dental exams every six months with panoramic X-rays. Aggressive preventive care — professional cleanings, fluoride, meticulous home hygiene.
Beyond Bones — Heart, Kidneys & Lungs
NOTCH2 signaling is involved in the development of the heart, kidneys, and other organs. The extraskeletal complications can be just as serious.
Cardiovascular Complications
Documented cardiac findings include patent ductus arteriosus, septal defects, and valve abnormalities. Romosozumab (Evenity) carries a black-box cardiovascular warning — if you have any cardiac involvement, this needs careful discussion.
Kidney Involvement — The SFPKS Connection
What used to be called serpentine fibula-polycystic kidney syndrome (SFPKS) is now recognized as the same condition as HCS. Polycystic kidneys in approximately 10% of patients, with at least one case progressing to end-stage renal failure by age 14.
Respiratory System
Three respiratory threats: thoracic deformities creating restrictive lung disease, recurrent respiratory infections, and basilar invagination compressing the brainstem causing central respiratory arrest.
Hearing & Voice Changes
A deep, gravelly voice is one of the recognized features of HCS. Hearing loss is more consequential. Both sensorineural and conductive loss have been documented, and in some cases the loss is progressive.
Annual audiometry is the only way to catch it before it significantly impacts daily life — especially in children, where undetected hearing loss affects speech and language development.
How HCS Changes Over Time
HCS is present from birth, but it doesn't look the same at every age. Different systems become affected at different life stages, and the condition generally worsens over time.
Birth – 2 yrsInfancy
Congenital features present at birth: cleft palate, congenital heart defects, open cranial sutures, wormian bones. Most children have normal mental development.
2 – 12 yrsChildhood
Skeletal manifestations become clinically apparent: short stature, joint hypermobility, early fractures, acro-osteolysis. Abnormal dental eruption and early tooth loss start. Facial features become more recognizable.
12 – 25 yrsAdolescence
Osteoporosis accelerates: vertebral compression fractures, progressive height loss, worsening kyphosis. Many patients are first diagnosed during this period. This is when bone treatment becomes urgent.
25+ yrsAdulthood
Progressive complications accumulate: continued bone density loss, ongoing acro-osteolysis, progressive hearing loss, worsening dental disease. Neurological complications may progress.
The age-dependent pattern is why early diagnosis matters — not because we have a cure, but because starting treatment earlier gives you the best chance of staying ahead of the progression.
Family Planning & Inheritance
HCS follows autosomal dominant inheritance.
50%Chance per
pregnancy
pregnancy
If one parent has HCS, each pregnancy carries a 50% chance of the child inheriting the NOTCH2 variant. This applies equally to sons and daughters.
However, many cases of HCS are de novo — meaning the mutation occurred spontaneously. If your child has HCS but neither parent does, the recurrence risk for future siblings is very low.
There is nothing a parent did to cause the mutation. This is not caused by anything during pregnancy.
Preimplantation Genetic Testing (PGT-M)
Families who wish to have children without HCS can use PGT-M. This involves creating embryos through IVF, testing each for the specific NOTCH2 variant, and transferring only unaffected embryos.
A genetic counselor is your best resource here. Ask your geneticist for a referral — or contact your provincial/state genetics program directly.
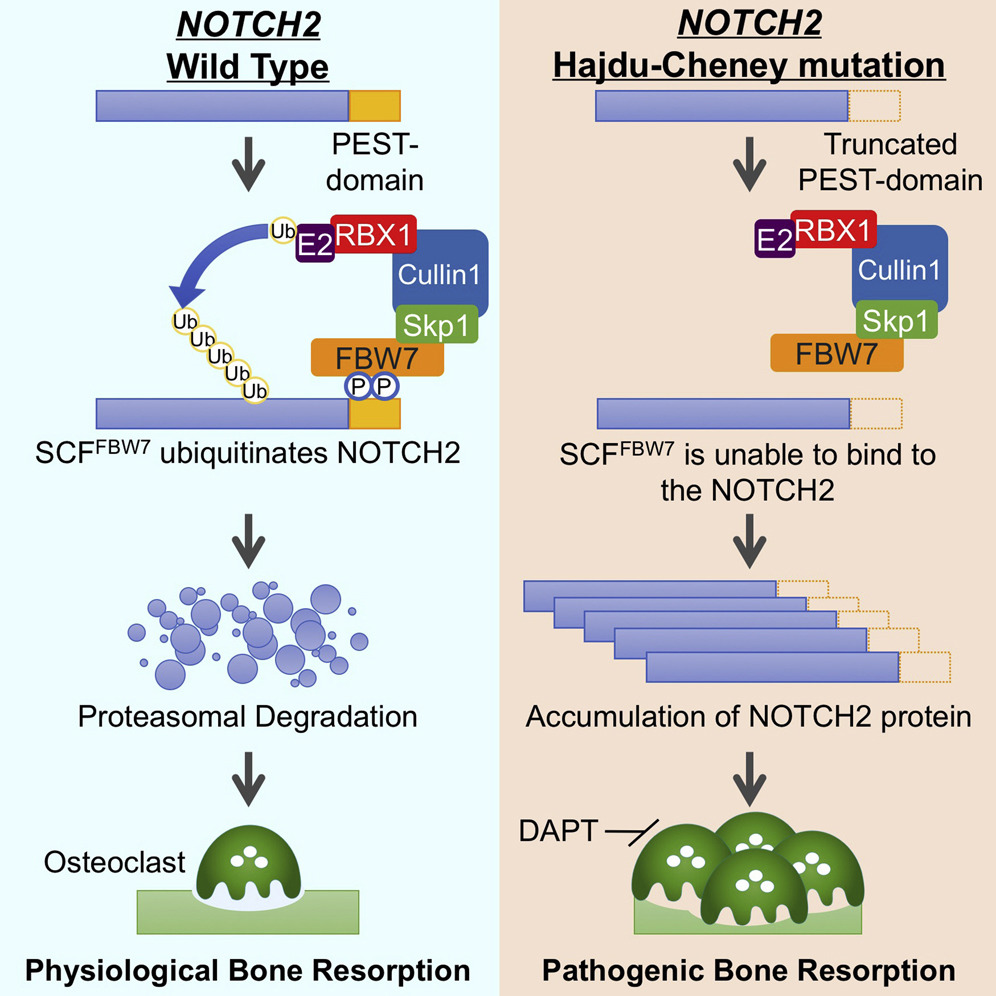
For more on the NOTCH2 pathway and preclinical research —
View HCS ResearchSources & Further Reading
This guide draws on peer-reviewed medical literature and trusted rare-disease databases. Because Hajdu-Cheney syndrome is so rare, much of what is known comes from case reports and small series — the sources below are where to read further and verify with your own clinicians.
- U.S. National Library of Medicine (NIH). Hajdu-Cheney syndrome. MedlinePlus Genetics. medlineplus.gov
- National Organization for Rare Disorders. Hajdu Cheney Syndrome. rarediseases.org
- Simpson MA, Irving MD, et al. Mutations in NOTCH2 cause Hajdu-Cheney syndrome, a disorder of severe and progressive bone loss. Nature Genetics, 2011. PubMed
- Hajdu-Cheney Syndrome: A Systematic Review of the Literature. NCBI PMC. PMC7504254
- Bisphosphonate therapy for spinal osteoporosis in Hajdu-Cheney syndrome — new data and literature review. Orphanet Journal of Rare Diseases, 2018. Orphanet J Rare Dis
- Craniospinal Surgery in Hajdu-Cheney Syndrome: A Review of Case Reports. NCBI PMC. PMC8763295
Last reviewed:
Community Voices
Stories and insights from the HCS community will appear here as they are submitted and reviewed. Be the first to share yours.
No stories yet — yours could be the first.