

“It is not the size of the tumor — it is the amplification of the signal.”
POEMS Syndrome
Polyneuropathy, Organomegaly, Endocrinopathy, Monoclonal protein, Skin changes
POEMS syndrome is a rare, life-threatening paraneoplastic disorder caused by a tiny clone of abnormal plasma cells. Despite its small tumor burden, this clone secretes massive amounts of vascular endothelial growth factor (VEGF) and other cytokines, creating a cascade of systemic damage across nearly every organ system. It is also known as Crow-Fukase syndrome, Takatsuki syndrome, and osteosclerotic myeloma.
POEMS now belongs to a newly defined category called Monoclonal Gammopathy of Clinical Significance (MGCS) — reframing it as a signaling disorder rather than a traditional cancer of bulk.
What the Letters Mean
The acronym captures the hallmark features — but the full clinical picture extends far beyond these five letters.
The VEGF Story: How a Tiny Clone Creates Systemic Chaos
A small clone of abnormal plasma cells — often just 5–10% of bone marrow — secretes massive amounts of vascular endothelial growth factor (VEGF) and other proinflammatory cytokines including TNF-α, IL-1β, IL-6, and TGF-β1. This single mechanism drives the full spectrum of disease.
Why POEMS Is Missed: The Diagnostic Odyssey
POEMS is among the most frequently misdiagnosed conditions in medicine. Each subspecialist typically sees only one system at a time — the full pattern goes unrecognized.
The most common misdiagnosis. Both cause demyelinating neuropathy, but POEMS has more severe axonal loss, prominent lower-limb atrophy, neuropathic pain, and does NOT respond to IVIG, steroids, or plasmapheresis the way CIDP does. Cranial nerve involvement and dysautonomia — common in CIDP — are rare in POEMS.
Both involve plasma cell disorders and M-proteins, but myeloma produces lytic ("punched out") bone lesions while POEMS produces sclerotic (dense) lesions. Myeloma has heavy tumor burden; POEMS has a tiny clone with massive systemic effects. Myeloma does not typically cause neuropathy unless amyloidosis is involved.
The M-protein in POEMS is typically small — often undetectable on serum electrophoresis in 30–46% of patients, and even missed on immunofixation in 15–25%. Hematologists may label it as MGUS and recommend watchful waiting — missing the systemic storm already underway. Serial measurements may be necessary.
- Neurologists see neuropathy → label CIDP
- Hematologists see small M-protein → say MGUS or watch-and-wait
- Endocrinologists treat the thyroid or diabetes in isolation
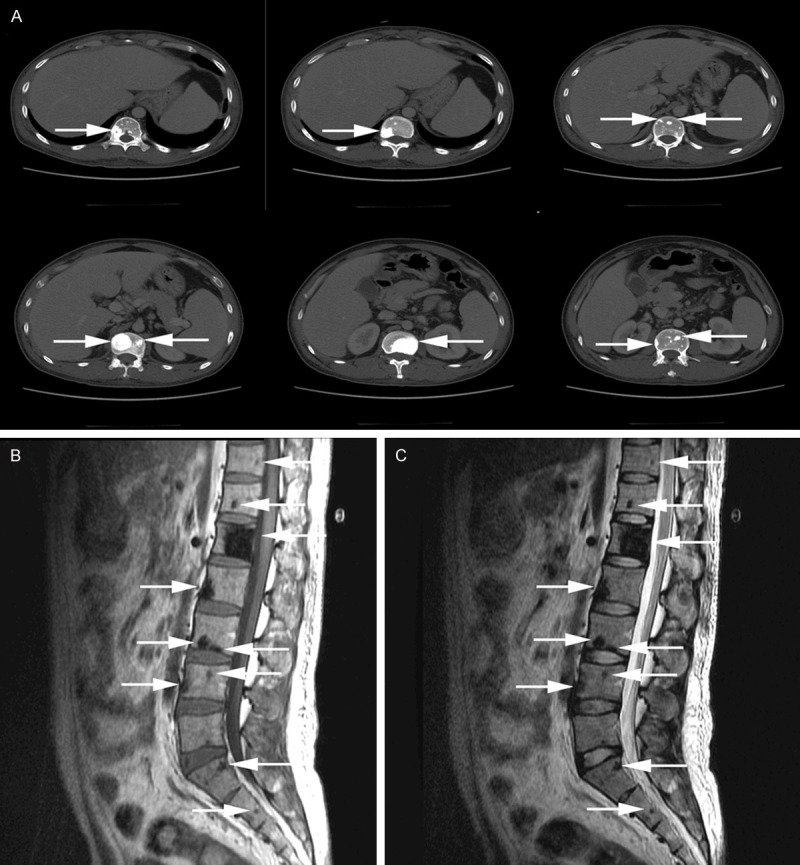
- Radiologists may miss sclerotic lesions unless specifically looking — CT with bone windows is far more sensitive than plain X-ray
- No single specialist sees the full picture — POEMS requires someone to zoom out and connect systems
🚩 Red Flags That Should Trigger Suspicion
- Neuropathy that does not respond to standard CIDP treatments (IVIG, steroids, plasmapheresis)
- Neuropathy plus thrombocytosis and/or polycythemia — these do NOT occur in CIDP
- Neuropathy plus unexplained edema, ascites, or pleural effusions
- Neuropathy plus endocrine abnormalities
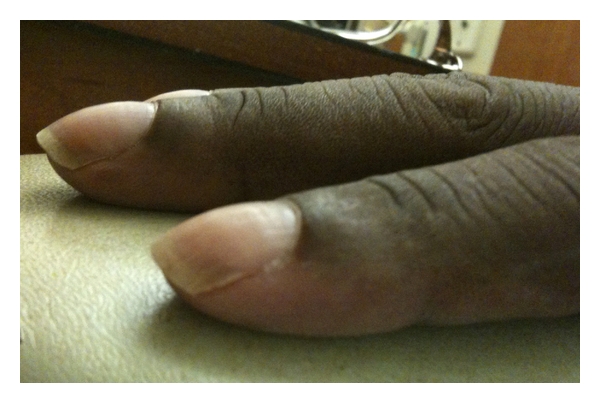
- Neuropathy plus skin changes (hyperpigmentation, white nails, clubbing, hypertrichosis)
- Any of the above with a lambda-restricted M-protein, however small
Complete Clinical Features
POEMS involves far more systems than the acronym suggests. Click each feature to expand.
Features in the Acronym
- Subacute, progressive, symmetric, length-dependent sensorimotor neuropathy
- Begins distally in the feet — numbness, tingling, burning, dysesthesias
- Progresses to proximal weakness; hands affected only after legs reach knee level
- Motor impairment eventually dominates sensory symptoms
- Painful neuropathy is common (unlike typical CIDP)
- Can progress to respiratory compromise if phrenic nerves are involved
- Bilateral foot drop and lower-limb atrophy are characteristic
- Nerve conduction: primary demyelination with secondary axonal loss — "uniform demyelination" distinguishes POEMS from the patchy demyelination of CIDP
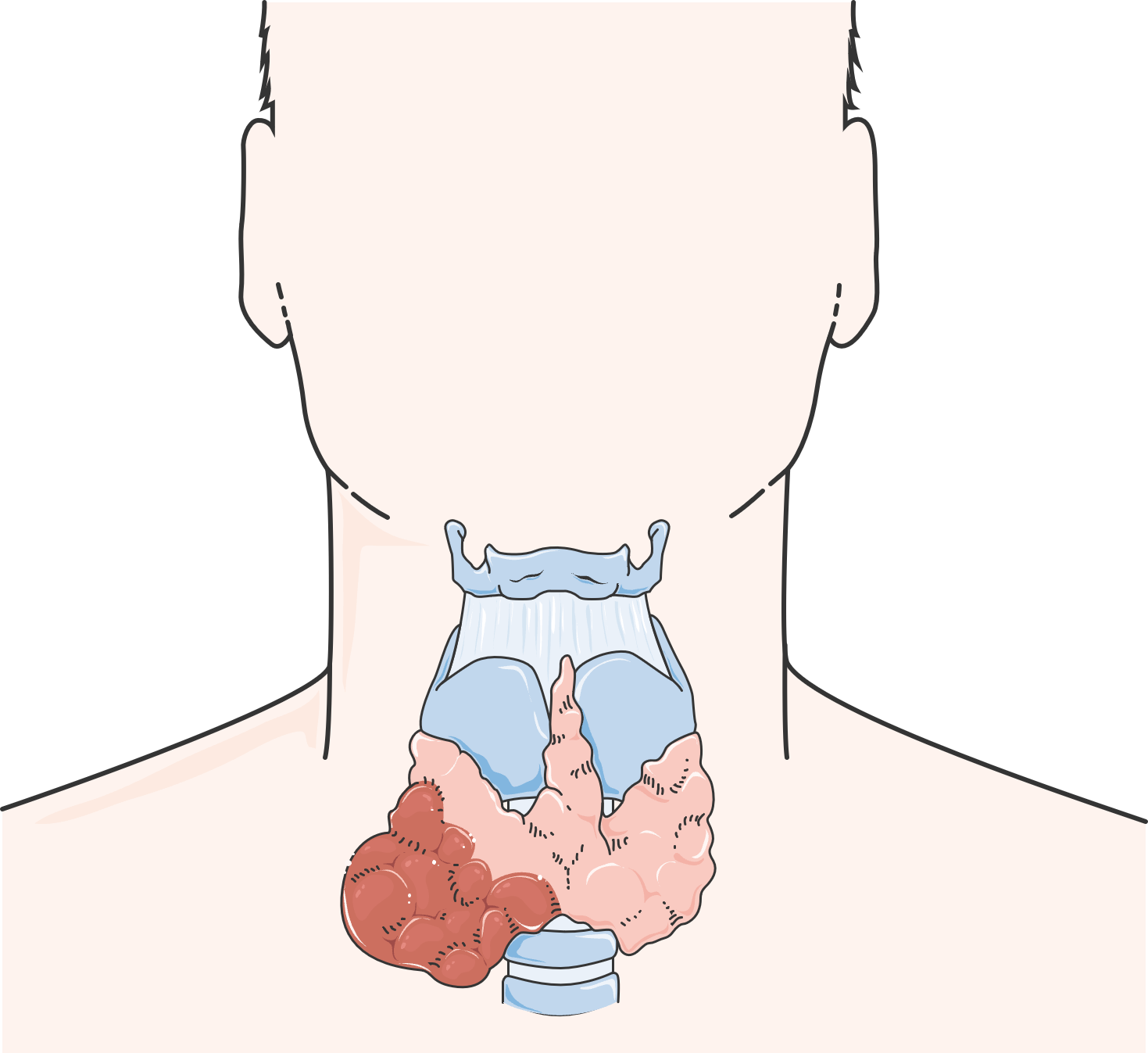
- Hepatomegaly, splenomegaly, lymphadenopathy — usually mild; bulky disease is uncommon
- Lymph node biopsy shows Castleman disease histology in 11–30% of cases
- Hypogonadism (most common) — erectile dysfunction, amenorrhea, gynecomastia
- Hypothyroidism
- Diabetes mellitus / glucose intolerance
- Adrenal insufficiency
- Hyperprolactinemia — newly identified as a risk factor for venous thrombosis
Note: Diabetes and thyroid abnormalities alone are excluded from minor diagnostic criteria due to high background prevalence.
- Almost always lambda light-chain restricted — this detail signals credibility to hematologists
- Typically IgA-λ or IgG-λ
- Characteristically small — often less than 2 g/dL
- Missed on serum electrophoresis (SPEP) in 30–46% of cases
- Missed on immunofixation in 15–25% of cases
- Serial measurements may be necessary — may not be detectable in early disease

- Hyperpigmentation (most common)
- Hypertrichosis (excessive hair growth)
- Skin thickening / scleroderma-like changes
- White nails (leukonychia)
- Digital clubbing
- Acrocyanosis
- Glomeruloid hemangiomas — highly specific for POEMS but rare
- Facial fat pad atrophy / facial lipoatrophy
Beyond the Acronym — Clinically Critical Features
Peripheral edema (most common), ascites, pleural effusions, pericardial effusions. Correlates with poorer survival. Often refractory to diuretics until the clone is treated.
A major and under-recognized complication. In the UCLH Registry (103 patients), 30% experienced at least one thrombotic event. Arterial events are slightly more common than venous — unusual for plasma cell disorders.
- Stroke accounts for 26% of all thromboses and 53% of arterial events
- Other arterial events: peripheral arterial occlusion, MI, microvascular disease, acute carotid obliteration, limb ischemia, bowel ischemia, Budd-Chiari syndrome
- Venous events: DVT, PE, PICC-associated DVT during ASCT
- Most thromboses occur BEFORE treatment starts — during active disease
Risk factors: thrombocytosis, elevated hemoglobin/hematocrit (especially men — 32% vs 5%), extravascular volume overload, splenomegaly, hyperprolactinemia (venous).
Far more common than previously recognized. At Peking Union Medical College, 27% of 154 patients had sPAP ≥50 mmHg at diagnosis. Other studies report 33–48%.
- Significantly worsens survival — median OS of 54 months with PH vs not reached without PH
- Reversible with successful treatment of the underlying POEMS
- Pathology is heterogeneous — plexiform lesions (PAH-like) or plasma cell infiltration of pulmonary arteries
- Cytokine-mediated: IL-1β, IL-6, TNF-α, and VEGF drive pulmonary vascular remodeling

- Can be sclerotic, lytic with sclerotic rim, or mixed ("soap bubble" appearance)
- Most common in axial skeleton — pelvis, spine, ribs, proximal extremities
- Most are less than 1 cm — CT with bone windows far more sensitive than plain X-ray
- ~50% have a single lesion; ~50% have multiple
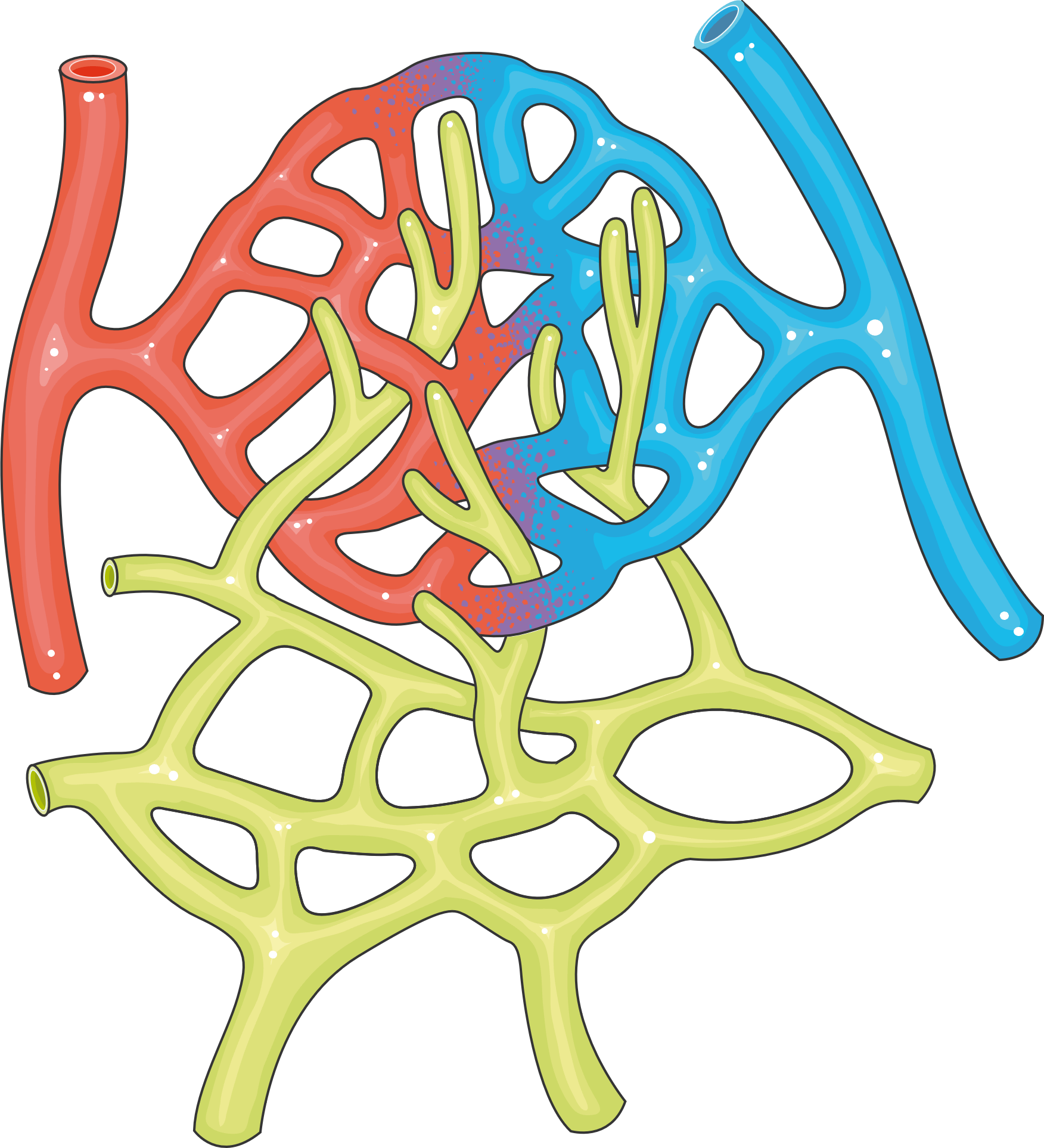
Not in diagnostic criteria but commonly seen on biopsy. Typical pathology includes MPGN-like lesions, mesangiolytic glomerulonephritis, or thrombotic microangiopathy. Electron microscopy shows glomerular microangiopathy with endothelial injury — the same endothelial damage found in nerve vasa nervorum, suggesting generalized endothelial injury is a unifying mechanism.
eGFR below 30 mL/min is an adverse prognostic factor. Can improve with bortezomib-based treatment.
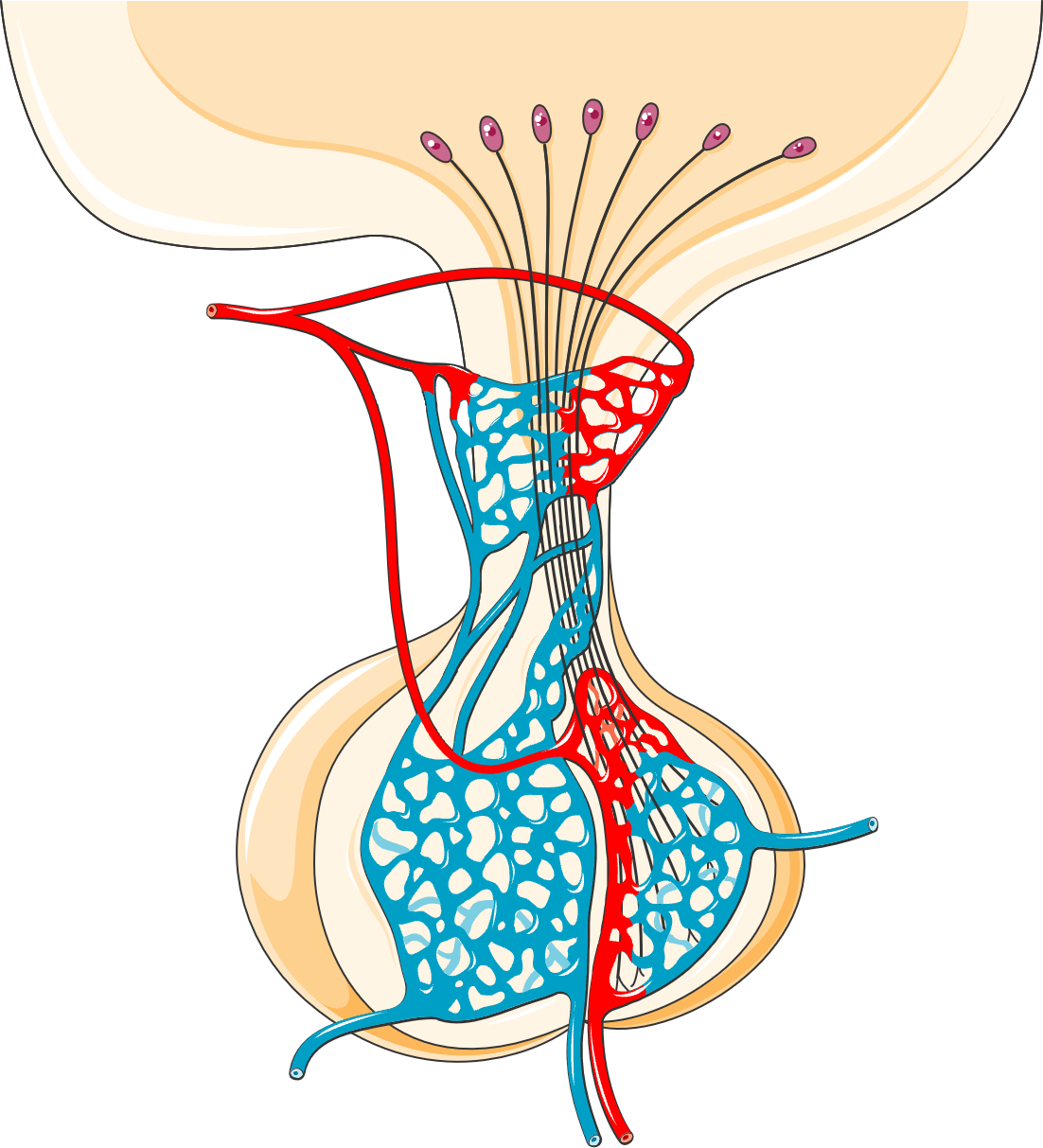
- Papilledema — optic disc swelling, can occur even without elevated intracranial pressure (VEGF-mediated)
- Thrombocytosis / Polycythemia — with neuropathy, should immediately raise suspicion for POEMS
- Left ventricular hypertrophy and subclinical cardiac dysfunction (systolic and diastolic)
- Sleep-disordered breathing
- Weight loss with facial fat pad atrophy
- Hyperhidrosis (excessive sweating)
- Low vitamin B12 levels
- Diarrhea
- Restrictive lung disease / decreased DLCO
- Elevated CSF protein with normal cell count
How Common Are the Features?
Prevalence of Clinical Features in POEMS Syndrome
Data compiled from Mayo Clinic, UCLH Registry, and Peking Union Medical College cohorts. Ranges reflect variation across study populations.
Formal Diagnostic Criteria
Dispenzieri / Mayo Clinic, Updated 2023. Diagnosis requires meeting ALL of the following groups.
Mandatory Criteria — BOTH Must Be Present
- Polyneuropathy (typically demyelinating)
- Monoclonal plasma cell proliferative disorder (almost always lambda light-chain restricted)
Other Major Criteria — At Least ONE Required
- Sclerotic bone lesions
- Elevated VEGF (often >1,000 pg/mL — but patients at ~850 pg/mL should not be excluded)
- Castleman disease
Minor Criteria — At Least ONE Required
- Organomegaly (splenomegaly, hepatomegaly, or lymphadenopathy)
- Extravascular volume overload (edema, pleural effusion, ascites)
- Endocrinopathy (excluding diabetes and thyroid disease alone)
- Skin changes (hyperpigmentation, hypertrichosis, glomeruloid hemangiomas, white nails)
- Papilledema
- Thrombocytosis / polycythemia
A recognized variant that occurs WITHOUT a clonal plasma cell disorder. Lymph node biopsy reveals Castleman histology and multiple POEMS minor criteria are present, but M-protein and/or polyneuropathy may be absent. These patients should be classified separately.
- Neuropathy tends to be more subtle and sensory-predominant
- High IL-6 levels
- Inferior overall survival compared to classic POEMS
- Youngest reported case: 6 years old — initially misdiagnosed as Guillain-Barré syndrome
- Complete blood count with differential
- Comprehensive metabolic panel
- Serum protein electrophoresis with immunofixation
- Serum free light chains
- 24-hour urine for protein electrophoresis and immunofixation
- Serum VEGF level
- Thyroid function tests
- Cortisol, testosterone/estradiol, FSH/LH
- Prolactin, HbA1c, IGF-1
- Bone marrow biopsy with immunohistochemistry
- CT (chest/abdomen/pelvis) with bone windows — NOT plain X-ray
- PET/CT if available
- Nerve conduction studies / EMG
- Echocardiogram with PA pressure estimation
- Pulmonary function tests including DLCO
- Fundoscopic examination
POEMS vs CIDP vs Multiple Myeloma
Pattern recognition is the key to diagnosis. These three conditions are most commonly confused.
| Feature | POEMS Syndrome | CIDP | Multiple Myeloma |
|---|---|---|---|
| Core Mechanism | Small clone → VEGF/cytokine excess | Autoimmune attack on nerve myelin | Malignant plasma cell proliferation |
| M-Protein | Lambda-restricted, often small | Usually absent | Often large (IgG, IgA, light chain) |
| Neuropathy | Severe, painful, uniform demyelination | Motor > sensory, patchy demyelination | Rare unless amyloidosis |
| VEGF Level | Markedly elevated | Normal | Normal |
| Bone Lesions | Sclerotic (dense) | None | Lytic (punched-out) |
| Organomegaly | Common | No | Uncommon |
| Endocrine Problems | Very common (multiple systems) | No | Not typical |
| Skin Changes | Hyperpigmentation, clubbing, white nails | No | No (unless amyloidosis) |
| Edema / Fluid | Common (80%) | No | Only advanced |
| Platelets | Often elevated | Normal | Often low |
| Red Blood Cells | Often elevated | Normal | Often low (anemia) |
| Thrombosis Risk | High (27–42%) — arterial + venous | Normal | Moderate (mainly venous) |
| Renal | MPGN-like; eGFR matters | No | Common (cast nephropathy) |
| Response to IVIG | No | Often responsive | No |
| Typical Age | 50–55 | Any adult | 65+ |
| 5-Year Survival | >80–90% | Chronic, managed | ~55% |
Quick Diagnostic Differentiators
Thrombosis in POEMS: The Under-Recognized Danger
Thrombosis — Types and Distribution
- Prophylactic antiplatelet therapy for ALL patients at diagnosis
- Low-molecular-weight heparin (LMWH) until VEGF drops below 1,000 pg/mL
- Maintain LMWH throughout IMiD therapy (lenalidomide, thalidomide)
- Consider full anticoagulation for high-risk patients: polycythemia, thrombocytosis, splenomegaly, prior thrombosis, effusions
Risk Stratification & Prognosis
✅ Favorable Factors
- Younger age
- Serum albumin >3.2 g/dL
- Complete hematologic response (CRH) — predicts 88% PFS even without maintenance
⛔ Adverse Factors
- Age >50
- Low serum albumin
- Pleural effusion
- Pulmonary hypertension
- eGFR <30 mL/min
- Fingernail clubbing
- Extravascular volume overload
- Decreased DLCO
- Clinical hypothyroidism
- Papilledema
Most frequent causes of death: renal failure, infection, and cardiopulmonary failure (including pulmonary hypertension). Secondary malignancies (particularly MDS) have been reported after alkylator-based or transplant therapies.
Treatment: The Revolution
POEMS is one of the most treatable rare diseases once correctly diagnosed. The fundamental goal is to eradicate or suppress the underlying plasma cell clone. When the clone is eliminated, VEGF plummets — often within weeks — and symptoms can reverse dramatically.
Radiation therapy alone — often curative. 10-year overall survival ~70%. Monitor closely for relapse or evolution to disseminated disease.
- Induction chemotherapy (typically bortezomib-based — CyBorD or similar, or lenalidomide + dexamethasone)
- Followed by high-dose melphalan conditioning + autologous stem cell transplant (ASCT) — the gold standard
- ASCT produces durable remissions — patients achieving CRH have PFS of 88% even without maintenance
- Transplant-related mortality: ~5% in pooled data
- Bortezomib-based regimens significantly improve neurological symptoms and kidney function
- Melphalan + dexamethasone (MDex) — conventional low-dose therapy
- Lenalidomide + dexamethasone (Ld) — 75–90% of patients symptom-free by 3 years
- Thalidomide + dexamethasone — the only agent studied in an RCT (J-POST trial); VEGF reduction was significant but 23% developed NEW sensory neuropathy
- Daratumumab + lenalidomide + dex (DRd) — emerging frontline option with rapid/durable responses; can enable transplant-ineligible patients to become candidates
Mayo Clinic Experience — the largest systematic report:
- Pomalidomide-based: Active but less data
- Elotuzumab-based: Responses observed (confirmed by Chiba University)
- Triplet regimens likely superior to doublets
- No treatment discontinuations due to adverse events; no deaths on therapy
- BCMA/CD3 bispecific antibody (CM336) — a clinical trial is evaluating this agent specifically for POEMS, based on 2025 Chinese Expert Consensus criteria
- Anti-BCMA CAR-T cells — case reports in POEMS/myeloma dual cases
- Ixazomib-based combinations (oral proteasome inhibitor) — trials ongoing
- Teclistamab — potential candidate given its BCMA-targeting mechanism
Neuropathy Recovery: What Patients Can Expect
This is what the POEMS community needs most — evidence that recovery is possible.
Mayo Clinic: 60-Patient ASCT Cohort (Median Follow-up 61 Months)
Mobility Aid Usage — Before vs After Transplant
- Muscle strength and gait typically improve steadily
- Sensory symptoms often improve but may take much longer
- Foot drop can take the longest to resolve
- Neuropathic pain may persist but usually improves
- Nerve regeneration at ~1 mm/day (~1 inch/month) — recovery from severe axonal loss is measured in months to years
- Physical therapy is critical — prevents contractures, strengthens muscles, relearns motor patterns
- Ankle-foot orthotics (AFOs) increase mobility and reduce fall risk during recovery
"We tell patients not to be discouraged. Nerves need time to regenerate." — Dr. Jack Khouri, Cleveland Clinic
Relief from neuropathy can begin as quickly as 2 months after effective treatment. Not all patients achieve full neurologic recovery — those with more severe axonal loss at diagnosis tend to have more residual deficits. This is why early diagnosis matters — less axonal damage means more recovery potential.
Supportive Care: The Details That Matter
Supportive care is not secondary — it is imperative to patient outcomes.
- All patients: prophylactic antiplatelet therapy at diagnosis
- LMWH until VEGF drops below 1,000 pg/mL
- Maintain LMWH throughout IMiD therapy (lenalidomide, thalidomide)
- Consider full anticoagulation for: polycythemia, thrombocytosis, splenomegaly, prior thrombosis, effusions
- Physical therapy — crucial for recovery and prevention of tendon contractures
- Ankle-foot orthotics (AFOs) — for foot drop, improving mobility and reducing falls
- Neuropathic pain treatment (gabapentin, pregabalin, duloxetine as appropriate)
- Assistive devices during recovery
- CPAP for sleep-disordered breathing or respiratory involvement
- Monitor DLCO and pulmonary function serially
- Consultation with endocrinology is essential
- Thyroid replacement for hypothyroidism
- Testosterone/estrogen replacement for hypogonadism
- Glucose management for diabetes
- Adrenal replacement if adrenal insufficiency is present
- Some endocrinopathies may be treatment-related rather than direct consequences of the clone
Diuretics for edema, ascites, and pleural effusions — but often refractory until the clone is treated. Drainage of large effusions if symptomatic.
- Serum VEGF every 3–6 months (the most useful biomarker)
- Nerve conduction studies periodically
- Imaging (CT/PET) every 1–2 years
- Echocardiogram for PA pressure monitoring
- Renal function (eGFR)
- Complete hematologic response assessment
Research & Community Timeline
Image Credits
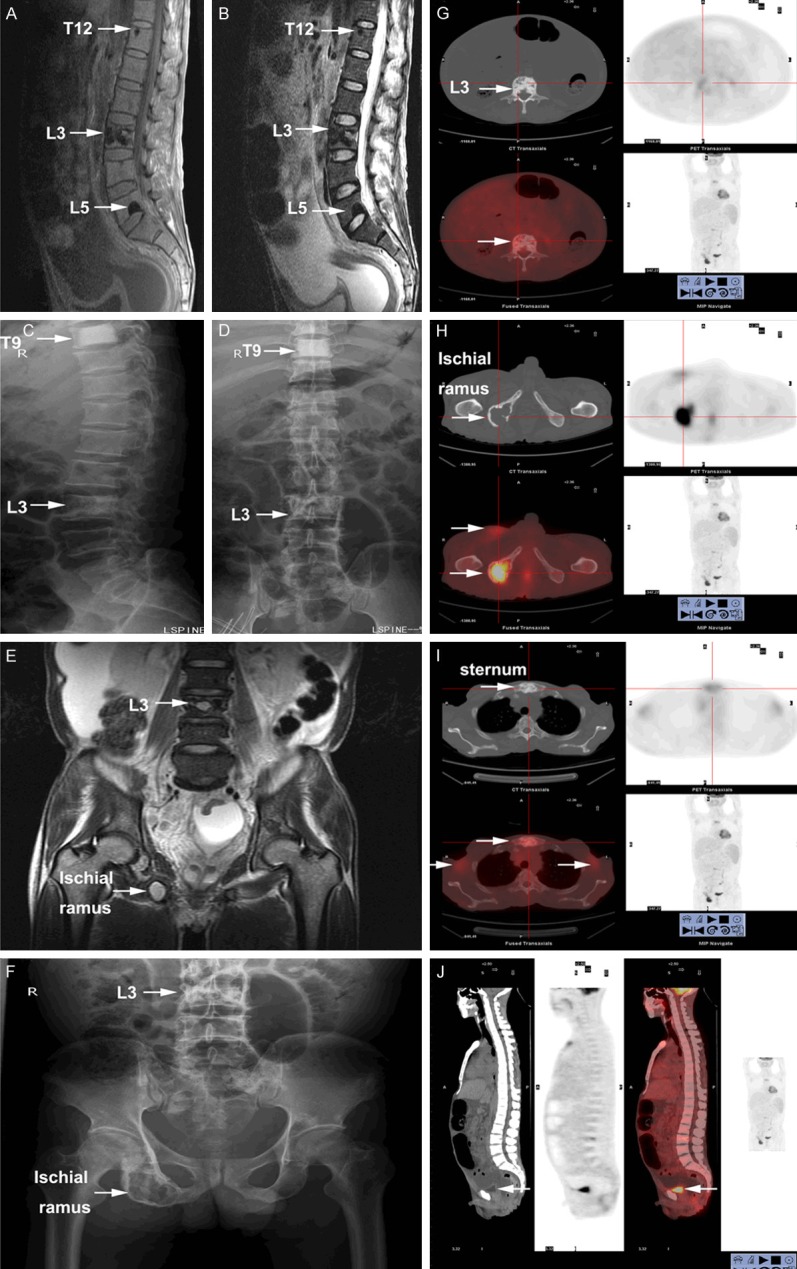
Clinical imaging: Shi XF et al., "Multimodal imaging and clinical characteristics of bone lesions in POEMS syndrome," Int J Clin Exp Med 2015;8(5):7467-76, PMC4509235. Chen YH et al., CCR3, PMC4831386. Case Reports in Medicine, PMC3195534. All images reproduced under Creative Commons licenses.
Medical illustrations: Servier Medical Art (smart.servier.com), licensed under CC BY 4.0.
Custom infographics: Created for Bare Your Rare (bareyourrare.org). Data sourced from Dispenzieri 2023/2025, UCLH Thrombosis Registry, Peking Union Medical College PH cohort, and Mayo Clinic treatment series.
Sources & Further Reading
This guide draws on peer-reviewed medical literature and trusted rare-disease databases. Because these conditions are rare, much of what is known comes from case reports and small series — the sources below are where to read further and verify with your own clinicians.
- Dispenzieri A. POEMS syndrome: 2023 update on diagnosis, risk-stratification, and management. American Journal of Hematology. Am J Hematol
- POEMS syndrome: diagnosis, treatments, and outcomes. ASH Hematology Education Program, 2025. ASH Education
- Orphanet. Diagnostic criteria for POEMS syndrome. orpha.net (PDF)
- National Organization for Rare Disorders. POEMS Syndrome. rarediseases.org
Last reviewed:
Community Voices
Stories and insights from the POEMS community will appear here as they are submitted and reviewed. Be the first to share yours.
No stories yet — yours could be the first.